











PD Dr. Jamila Andoh
Department of Psychiatry and Psychotherapy, Central Institute of Mental Health, Medical Faculty Mannheim, Heidelberg University
Prof. Dr. Dr. h. c. Dr. h. c. Herta Flor
Institute of Neuropsychology and Clinical Psychology, Central Institute of Mental Health, Medical Faculty Mannheim, Heidelberg University
Neural circuits involved in phantom limb pain
Intervention for PLP using combined virtual reality and brain stimulation with concurrent ecological momentary assessments
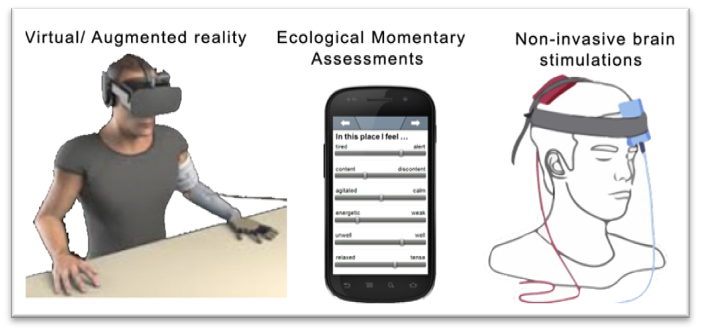
During ongoing PLP, we observed neural alterations in the insula, ACC and S1. Alterations in neural oscillations were also reported in the beta and gamma frequency bands. We now apply non-invasive brain stimulations combined with virtual reality to modulate altered neural activity, and PLP-specific neural oscillations.
To permit a fine-grained analysis between changes in PLP and contextual variables, we also assess daily changes in pain in the phantom and in the residual limb as well as other types of pain, psychological variables (e.g., anxiety, depression, stress, social responses to pain, body representation), use of prosthesis and of the intact limb employing ecological momentary assessment.
We assume that these fluctuations can be predicted by environmental and perceptual variables.
This study should give major insights into core modulating factors of PLP as well as optimised and individualised treatment approaches for PLP and help us determine to what extent peripheral changes interact with treatment success.
Bedside assessment of pain-related brain circuits and other predictive variables of phantom limb pain in amputees before and after the amputation
In the longitudinal study, we found evidence that pain before the amputation as well as psychological factors such as anxiety and depression best predict the presence of PLP one year after an amputation. We found decreased neural activity in the primary somatosensory cortex in all amputees over time. In amputees with PLP, we observed increased activity in the insula and in amputees without PLP, we found decreased activity in the anterior cingulate cortex over time. We did not find significant differences between amputees with and without PLP at early stage after amputation. This suggests that the changes observed may be a consequence of PLP rather than an antecedent.
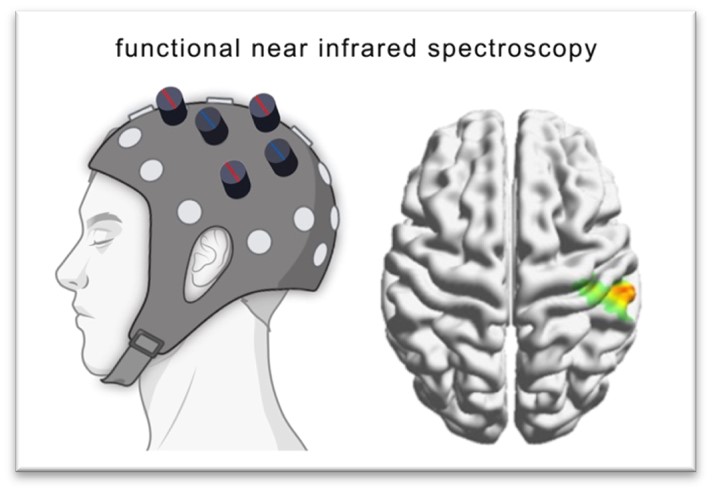
We now examine diabetic patients at risk for amputation and follow them post amputation to determine central and peripheral as well as psychological predictors of both amputation and PLP. This study is facilitated with bedside functional near-infrared spectroscopy (fNIRS). We expect that both hypo- and hyperexcitability of pain-related brain circuits may contribute to later PLP and expect to identify relevant factors of PLP.